




Body Fat Percentage Comparisons For Men & Women [2023 updated]
Nowadays the golden standard by which many health and fitness enthusiasts use to gauge their level of fitness is their body fat percentage. Ask just about anyone that is seriously into their training what their body fat percentage is, and quite often they can tell you exactly what it is to the nearest decimal point! When I started my training as an apprentice trainer over 30 years ago back in the islands, my coaches frowned upon the use of skinfold calipers and body fat testing in general. While the training manuals might have said that it was important to measure your client’s body fat percentage as an indicator of their progress, my coaches all said that if a client couldn’t look in the mirror and see visible differences in their body or how their clothes fit then I wasn’t doing my job. In my practice as a personal trainer in New York City and now in my role an online personal trainer my philosophy remains the same. At the end of the day, a change in numbers means nothing if your client still has layers of fat obscuring their midsection and no one walks around on the beach with their body fat percentage numbers printed out on their swimsuit! (See my article diet vs training- what matters most for body transformation.) There are also some very considerable limitations to field methods of body fat testing that make it somewhat impractical and so I have never used it in my personal training practice. That said, it is a good idea to have a ballpark idea of what your body fat percentage is for health reasons more than anything else, unless you are an athlete involved in distance events where weight to power ratios are all important, and you need to know just how far down you can go body fat wise without affecting your performance. In this article we are going to take a look at what men and women tend to look like at different body fat percentages and the various methods of measuring body fat- and their limitations. Thanks for reading and as always, be sure to share this article with someone who you think might find it to be of interest!
Body Fat Percentage Comparison: What Is A Healthy Body Fat Percentage?

Healthy body fat percentages vary based on age, gender and activity levels but you don’t have to be ultra lean with extremely low body fat to be healthy.
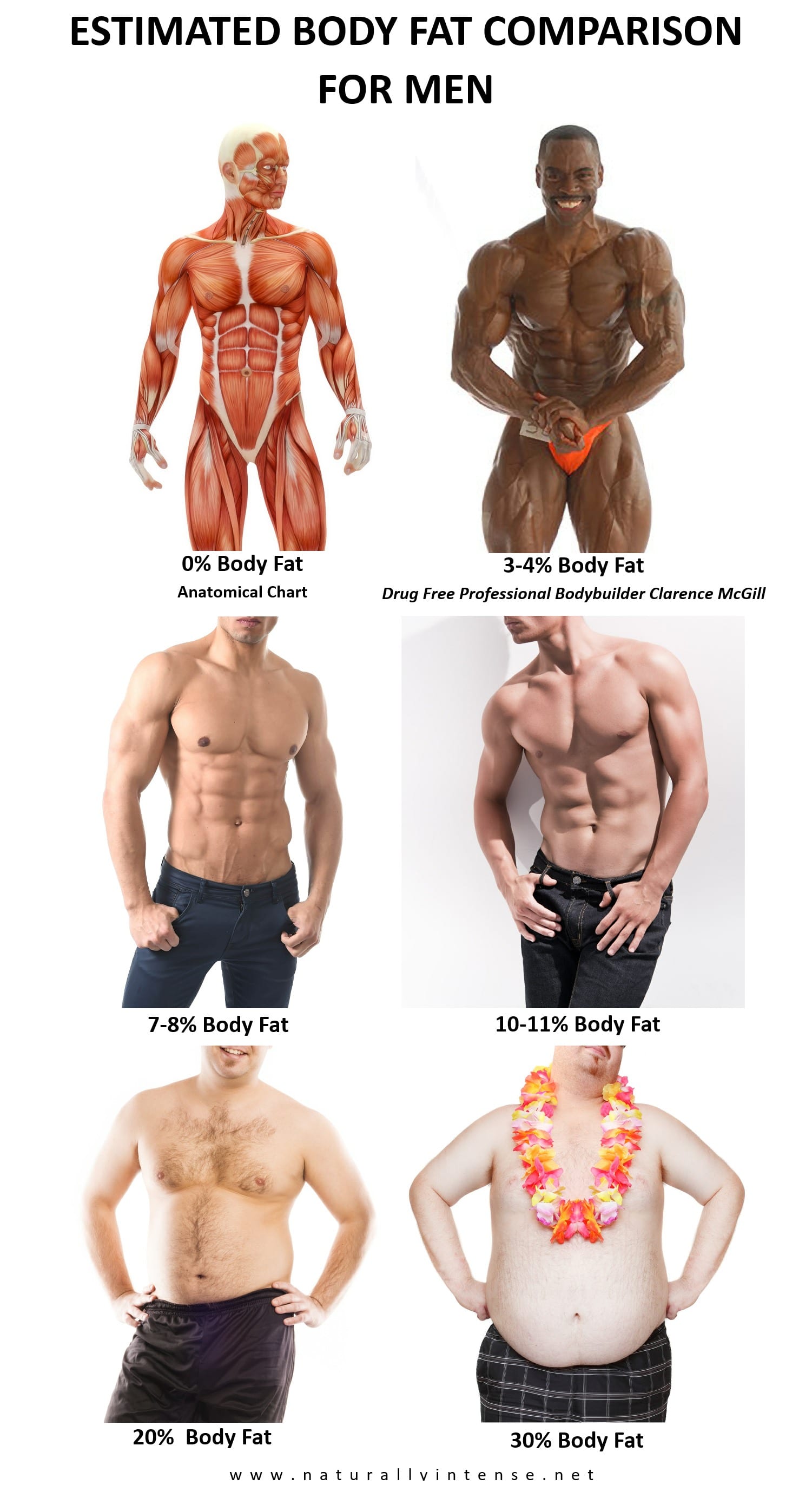
Most standards of ideal body fat percentages are far more cosmetic than anything else. For example, many bodybuilding and physique competitors describe themselves as ‘fat’ at body fat percentages far below what most people would kill to achieve. Athletes who take part in sports and activities where how your body looks is often considered almost as important as performance such as dance, diving, gymnastics and figure skating also can feel pressured to drop their body fat to levels even when their current weight and body mass is excellent in terms of health and optimal performance. That said, there are some loose standards of what a healthy body fat percentage generally should be, (as it varies at the lower limits based on the individual),- The American Council on Exercise recommends a body fat percentage of 6-25% for men and 14-31% for women while The American Dietetic Association recommends that men should be 15-18% body fat and women 20-25% body fat. For high level athletes, body fat percentages can vary from sport to sport but are usually lower than average. Healthy male athletes may have body fat levels as low as 5-12% body fat, and healthy female athletes can at times be as low as 12-20%.[36] Competitive bodybuilding requires having the appearance of having as little body fat as possible and male competitors are often reported to go as low as 3-4% with females can getting as low as 8-9%. These numbers however are always estimates as current testing cannot accurately measure such low body fat extremes.[35] You would think that the lower your body fat the healthier you would be but studies have shown that there is no added health benefit when men reduce their body fat under 8% and women drop their body fat under 14%.[37]
Body Fat Percentage Comparison: How Low Is Too Low?
Body fat is an important component for our overall health as it serves some very important roles as it acts as an insulator to help our bodies conserve heat, it helps cushion and protect vital organs and fat plays a key metabolic role in the production of energy for everyday activity. We generally have two different types of fat-
Storage Fat- which is stored under our skin, (subcutaneous fat), and for most males 12% of body weight is storage fat and for women 14% of body weight is storage fat.
Essential Body Fat- which is needed to keep us alive and maintain proper hormonal and reproductive function. While storage fat levels for men and women are similar, essential fat levels are quite different as men have about 3% of total bodyweight while women have 13%.
Since fat is such an essential part of what keeps us healthy and alive, training and dieting to drop body fat levels under healthy amounts not only leads to a decrease in performance, but can also create vitamin and mineral deficiencies, fluid and electrolyte imbalances, an increased risk of bone fractures, suppress the immune system, adversely affect reproductive functions and damage the heart.[38,39] I can tell you from personal experience as well that while having a body fat percentage in the very low single digits might look great, you pretty much feel really awful as the numbers start to go down. You feel cold all the time, your joints tend to hurt more than they usually would, you tire quickly and you don’t sleep as well either. Not as glamorous as it seems and to be honest, most people are much happier with a body fat percentage that is low- but not too low as it does cut down on your quality of life. (See my article: Ultra Low body Fat Isn’t Healthy- The Downsides Of Being Ripped). On the other end of the spectrum, high body fat is of course very much problematic. Body fat percentages above 25% for women and 20% for men are associated with a greater risk of developing cardiovascular disease, diabetes and certain cancers [40,41,42,43,44,45,46,47] and while you don’t need to have a body fat percentage in the single digits to be healthy it is important that the numbers don’t get too high.
Body Fat Percentage Comparison For Men & Women
What do the various body fat percentages actually look like on a real person? To start, most guys with muscle definition that you would call ‘cut’ or “ripped” tend to fall somewhere between 7-12% body fat. Most of the women who display a tight and toned physique, (not the skinny fat look), and who would be considered fit are usually are in the vicinity of 12-18% body fat. That said there are exceptions, as my experience has been that two people can have exactly the same body fat percentages yet look as different as night and day. Some people can have rippling abs with 15% body fat whereas others have to go as low as 6% to start seeing real definition in their abdominal muscles because of differences in where they store fat, (which is a genetic factor- see my article on Why People Store Fat In Different Parts of the Body) and levels of hydration. Bodybuilders, for example, who perhaps have the lowest body fat percentages, achieve their skinless look through a combination of dehydration and depleting body fat stores- as how much water you are holding can make a huge difference in how you look when body fat levels are extremely low. A male bodybuilding competitor could be ripped while dehydrated at an extremely low body fat level and after a few hours of eating high sodium foods would retain a significant amount of water that would make them appear bloated and with far less muscular definition. Except they would not have put on any additional body fat in such a short space of time and so their body fat percentage would be the same. The following images will give you a somewhat of a ballpark idea of what different body fat percentages look like on men and women.

Body Fat Percentage Comparison: Limitations Of Body Fat Testing
Before we delve into the various methods of measuring body fat percentages, it’s important to note that all methods are for the most part indirect and subject to error. 100% accuracy in measuring body fat is simply not possible without cutting someone up into pieces and physically measuring each piece. Since we’d rather know our body fat percentages while we are still in one piece the science is kind of like someone trying to figure out what’s inside a box without being able to actually open the box. We can make assumptions based on what can be measured outside the box, but at the end of the day we can’t always be 100% certain since we must rely on assumptions. The same applies to the equations used to calculate body fat percentages as they are all are based on theoretical models of that divide the body into, (usually), two components of fat and fat free body mass.[1,2,3] The fat mass encompasses all the lipids from adipose and other tissues while the fat free body mass includes water, protein and minerals. These models assume that the densities and relative proportions of protein, water, and minerals in fat free body mass are the same for everyone and that individual differ from the referenced ‘body’ only in the amount of fat they carry.[1,2,3] These assumed models are used to calculate body fat percentages from readings from advanced forms of body fat testing such as bio-impedance testing, air displacement testing, hydrostatic weighing and dual x-ray absorptiometry.
Research has shown that the assumptions made in these models do not always hold true for all groups. For example, fat free body mass densities can be significantly different due to gender, levels of muscularity, activity levels and ethnicity. [4,5,6] Malnutrition, obesity, osteoporosis as well as certain diseases can change the relative proportions of water and or minerals in fat free body mass[49], which could lead to errors when estimating relative body fat. So while some of the more involved methods of measuring body fat may be able to accurately measure total body mass, they may not be as accurate in determining body fat as they are limited by the formulas and assumptions they rely on for these calculations. (On a side note, formulas for skinfold caliper testing do take differences such as ethnicity and activity level into consideration, but have their own set of limitations which we will discuss later on in the article.)
How much of a margin of error are we talking about? In the vicinity of almost 3% according to some researchers [5] with hydrostatic weighing which is often used as a measure of accuracy for other forms of testing. On a purely cosmetic level, such a discrepancy is relatively insignificant but could be some cause for concern for an athlete trying to figure out how to keep their body weight as low as possible without adversely affecting performance. Precision for this group would be paramount- as a nearly 3% error margin could make the difference between winning and losing a highly competitive event where power to weight ratios make all the difference. That said, let’s take a look at some of the methods used to determine body fat percentages.
Body Fat Testing: BMI Charts
BMI charts are not accurate with athletes. If we went only by BMI charts at 6 feet tall and 225lbs I would be clinically obese! -Author & natural bodybuilder, Kevin Richardson.
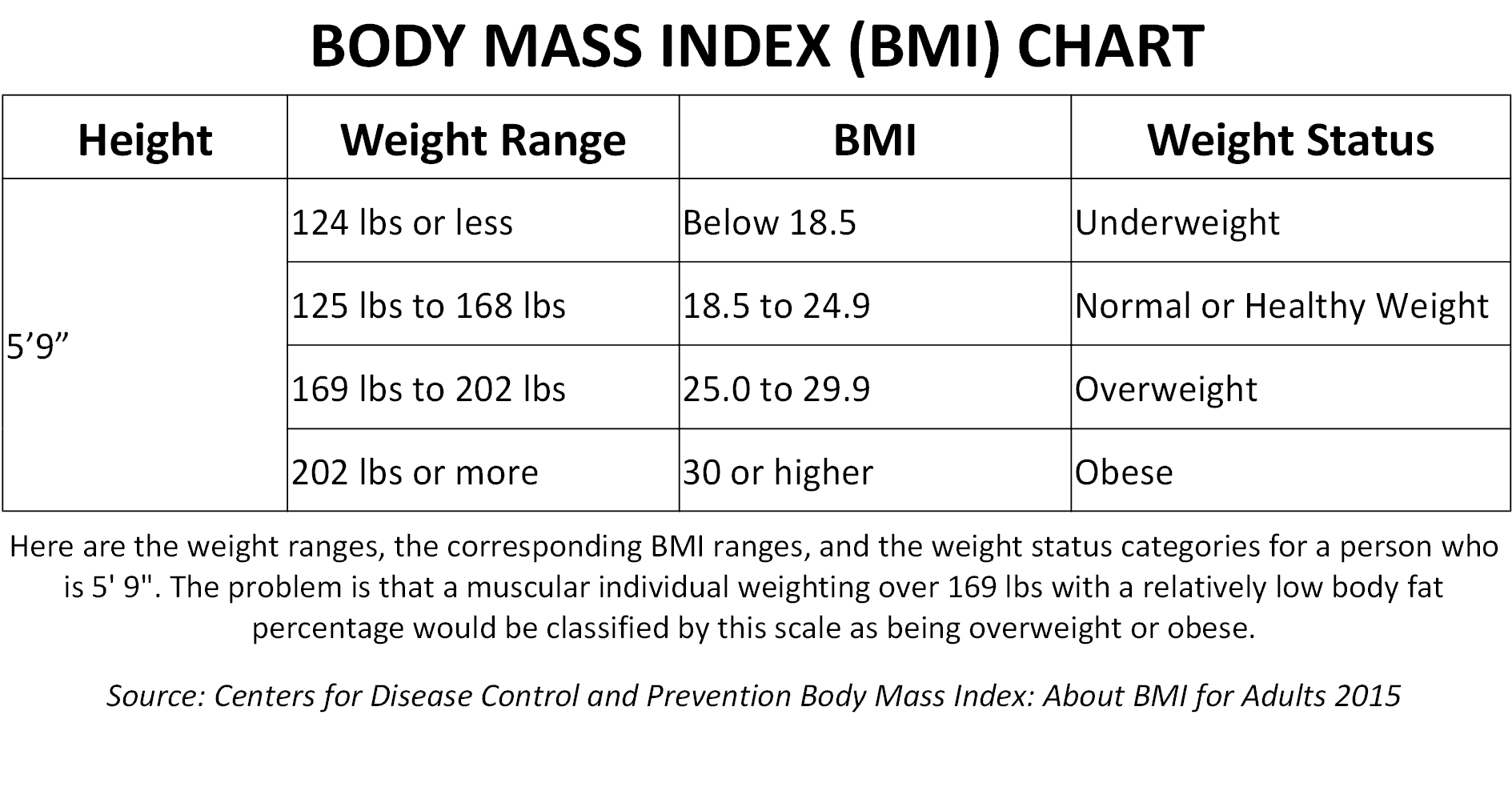
While not a true method of measuring body fat percentages, Body Mass Index (BMI) is perhaps one of the most popular method of informally measuring body composition. BMI is a measure of your bodyweight calculated in kilograms divided by the square of your height in meters(kg/m2)[1], in essence, it is a simple and noninvasive method designed to determine excess weight- not necessarily excess fat and the numbers do not always hold true for everyone. That said, numerous studies have validated the effectiveness of BMI testing as an indicator of increased risk of various metabolic diseases and health risks and that high BMI status is strongly correlated with higher body fat for most of the population.[7,8,9,10,11,12] It is a cheap and simple way to screen for health risks at the population level and allows health care professionals to easily categorize and make comparisons for health risks across various regions, times, and subgroups.[13]
There are, as we said, limitations on the individual level, as two people can be the same height and weight, (and thus have the same BMI), but be totally different from each other in terms of body fat percentages and health risks.[14] I remember when I enlisted in the U.S. Navy, (I was 20 years old at the time), and showed up at the recruiter’s office weighing in at a solid 220 lbs at a height of 6 feet tall. After stepping on the scale, they punched in some number on the calculator, pulled out a chart and told me that I was significantly overweight and would have to lose at least 30 to 40 lbs before I could enlist. My BMI was 29.8, which gave me a reading placing me on the higher end of being overweight and almost obese. I couldn’t tell you how funny this was as I had a body fat level at the time of about 8-7% at the time- with rippling abdominals and barely any fat readily visible on my frame. When I stripped down so the recruiter could see what I looked like under my clothes, he was shocked! (It was my first winter in the United States and coming from Trinidad I had a lot of layers on!) Needless to say I had nothing to worry about and I was able to enlist but this would be a story that would play itself out over and over in doctors’ offices before they had a chance to see what I actually looked like. Twenty years later at 225 lbs. and at a body fat level of maybe somewhere around 9-10% and with abs still rippling, according to BMI measurements, I am now officially obese, which really highlights the limitations of the BMI scales for muscular individuals and it has been acknowledged that athletic individuals can’t be accurately measured using BMI scales.[13,15] There are other recognized limitations to BMI scales, women generally tend to have higher body fat percentages than men with the same BMI.[15] Individuals of African descent tend to have lower levels of body fat that whites with the same BMI,[16,17] and Asians tend to have higher levels of body fat than white men with the same BMI.[18]
Body Fat Testing: The Tape Measure Method-Anthropometry

Tape measure methods of body fat testing are easy but not as accurate as other methods.
Another simple method of testing body fat is the tape measure method or anthropometry which involves taking measurements at various parts of the body and using a formula that also includes body mass and standing height to determine body fat and fat free mass.[23,24] It is relatively accurate when measurement are taken by a skilled technician but with tape measurements, people who are muscular and with low body fat levels can get numbers 3 to 5 percent higher than their true percent body fat percentages. Again, since the theoretical models used to calculate body mass assume that fat free mass and fat densities are constant for everyone[3,25,26] which is not, [27,28,29,30,31] there is always going to be a margin of error. Especially with individuals at the lower end of the spectrum. So, what’s the bottom line? For many people, the tape measure test is enough to give you a basic idea of your body fat percentages and it can be done frequently at little or no cost but don’t expect exacting accuracy.
Body Fat Testing- Skin Fold Calipers- The Pros and Cons

Many personal trainers include skin fold caliper testing as a way to determine their client’s body fat percentage and their progress. With skin fold testing, calipers are used to pinch select parts of the body after which the individual’s body fat is determined based on the assumption that the amount of fat stored at these various sites is proportional to a person’s overall body fat. Studies have found skinfold testing to be a reasonably reliable test for measuring body fat percentages when performed by a skilled technician- comparing well with more direct methods such as computed-tomography measurements. [5] For an expedient method to measure body fat, skinfold calipers offer a quick and relatively non-invasive way to determine body fat in the field and unlike some more sophisticated tests, the formulas used are population specific and thus can be used to accurately measure body fat percentages in individuals from various ethnic groups, (Black, Hispanic and White), as well as make adjustments for both male and female athletes.[49]
That said, there are some limitations to skinfold testing. It takes a significant amount of time and practice to be able to properly administer a skinfold test and very precise procedures must be followed in order to get a good reading.[33] The type of calipers used are also important as high quality metal calipers have greater scale precision than the cheaper plastic ones often used in gyms, and the plastic models are far more prone to error when administered by those who have not been rigorously trained.[34] Another limiting element is that skinfold calipers are not always able to measure the body fat of obese individuals, who sometimes have skin that is so thick that it exceeds the maximum aperture of the calipers. Time of testing is also important. Many trainers in gyms take measurements after their client’s workout to gauge progress but exercise, (resistance training in particular), can substantially increase intracellular fluid and thus adversely affects the accuracy of measurements from both tape and skinfold caliper tests that rely on skinfold thickness.[49] In general, however, skinfold calipers are not the best way to track ongoing progress if you are doing any type of resistance training.[19] Muscle tissue compresses the intracellular spaces between fat cells as it grows[20], so the total amount of subcutaneous fat in any part of the body that has experienced some degree of muscle growth can remain the same but occupy less space because of the increase in muscle mass. Skinfold calipers would measure this as a decrease in subcutaneous fat while a more involved scan such as an MRI, DEXA or CT scan would show no such changes at all.[20] Equally problematic is the increased water retention (edema) that can occur for days after a high intensity workout which could further skewer results. There are other constraints to consider; skinfold calipers measurements are only taken at the belly of the muscle, so any changes in subcutaneous fat in other parts of the pinched muscle group go undetected. Studies involving before and after measurements of men and women involved in a 16 week program of resistance training found no changes in subcutaneous fat when assessed by skinfold calipers. However, researchers did find significant reductions in body fat when assessed by magnetic resonance imaging, computer X ray tomography and dual x ray absorptiometry.[21,22] The studies concluded that short term decreases in subcutaneous body fat from resistance training can only be accurately detected using MRI, CT and DEXA techniques and assessments from skinfold tests.[21,22] That being said, while skinfold calipers may have a range of uses, it is a tool that I employ in my own personal training practice.
Bioelectrical Impedance Testing
Scales and hand held models for bio-impedance testing are not as accurate as the systems that allow for full body testing.
True bio-electrical impedance testing is far more involved, (and more accurate) than the more common methods in scales you have at home, at the gym or devices you can hold to measure body fat percentages. The way it works is that a small electrical charge is sent through the body, (arms and legs), and the individual’s total body water levels are estimated from impedance measurements. The greater the resistance, (measured in ohms), to the current flow, the more fat is present since fat tissue is a poor conductor of electricity due its low water content. The lesser the resistance, the more fat free body mass is present as non-adipose tissue is highly conductive due to its high water content.[34,51] These tests have been found to be relatively accurate when a current is sent through the whole body. In some ways bio-electrical impedance testing is easier than a skinfold tests as it can measure the body fat of obese individuals and does not require as much skill in order to administer the test. That said, there are some limitations as it can only be accurately administered if the subject has not eaten or had anything to drink within four hours of the test, has not used any type of diuretic medication within seven days of the test and it is not recommended for women who are retaining water due to their menstrual cycle.[49] You also have to urinate within thirty minutes of being tested and most importantly for those using this form of testing to determine the progress of their training program, you must not have exercised within twelve hours of the test.[49]
That said, segmented bio-impedance instruments such as scales that send a current through only the lower body and hand held devices that send a current only through the upper body, cannot fully measure total body water levels, only estimate them based on the part of the body that they do measure. There can be considerable discrepancies among individuals in terms of differences in fat free mass in the upper and lower body so only measuring one segment of the body introduces a margin of error. The use of scales and hand held devices may be popular among many trainers and gyms, (and are very often used after a workout in contradiction to the very strict usage guidelines), but their accuracy has never been validated the way full body bio-impedance has been with numerous independent studies, thus readings will always be questionable at best.
Advanced Body Fat Testing- The Pros & Cons of Hydrostatic Weighing

Hydrostatic testing, (or hydro-densitometry), for years has been the golden standard for body fat testing. It is a very involved and somewhat extreme procedure to say the least. It works on the precepts of the Archimedes principle which states that the upward force, (buoyancy), exerted on a body immersed in a fluid, whether fully or partially submerged, is equal to the weight of the fluid the body displaces. Since both bone and muscle are denser than water, (and would sink), a person with a high percentage of fat free mass, (like an athlete), will weigh more in the water because of their lower body fat percentage. On the other hand, fat tissue is less dense than water, (and would float) so a person with a large amount of fat mass will weigh less in the water because of their higher body fat percentage. I can attest to this myself as I can literally stand on the bottom of a pool and have a very hard time floating in general!
To perform the test you are first weighed in on dry land, then completely submerged in a tank of water while sitting on a scale designed to measure your underwater weight. The air in your lungs can significantly increase buoyancy and thus throw off the readings and so you have to expel as much air as is possible and remain completely still while your underwater weight it measured. This process is repeated no less than three times for accuracy purposes taking into consideration water temperature and the residual amount of air in your lungs, after which a special formula is used to gauge fat free weight and fat weight and determine your body fat percentage.[52,53,54] Not exactly a great way to spend your afternoon, and it is most certainly not for children, the elderly, people with physical challenges of any kind and the claustrophobic. Hydrostatic weighing does however can give a very precise reading of total body mass if the subject is able expel air comfortably underwater, and the residual air in the lungs is measured. However, while it is more accurate than caliper tests or tape measurements, it still has some degree of error. Hydrostatic weighing is limited by the formulas used to calculate body fat percentages. And as we said earlier in the article, these formulas are based on the assumption that the density of fat free mass is same for everyone and this assumption does not hold true for people of different races, genders, ages and activity levels.[4,5,6,49] It also cannot account for air in the intestines which can also have an effect on buoyancy, but you work with what you have and this is a very reliable method of testing.
Advanced Body Fat Percentage Testing- Whole Body Air Displacement Plethysmography (ADP)

Offering an even less invasive but advanced form of body fat testing is air displacement plethysmography which measures total body density and body volume. In order to do the test, the subject is placed inside a sealed chamber called a Bod Pod and body volume is calculated by subtracting the volume of air inside the chamber when the subject is in it from the volume of air in the chamber when it is empty. Boyle’s Law states that the product of the pressure and volume for a gas is a constant for a fixed amount of gas at a fixed temperature, so conditions inside the chamber are kept at a stable temperature and the pressure is changed in order to determine total air volume. The entire test takes less than 5 minutes and its accuracy is comparable to that of hydrostatic weighing in adults.[60] The speed and convenience of this form of testing makes it appealing for children, the elderly and the physically challenged, but like all tests it does have limitations. Studies have found that air displacement plethysmographs tend to overestimate the average body fat percentage of African Americans and underestimate the body fat percentages of football players. [61,62] It also has accuracy issues at the extreme ends with very lean and very obese individuals and of course is subject to the same error margins as hydrostatic weighing as it uses the same conversion formulas.[49]
Advanced Body Fat Percentage Testing- Dual-energy X-Ray Absorptiometry (DEXA)

Dual-energy X-Ray Absorptiometry or DEXA is a relatively new method of measuring body composition. It measures total body mineral mass, mineral free lean mass and fat tissue mass through the emission of two different types of X-ray radiation, (in a very small dose, of course) and measurement of the differences in absorption of the two energies. DEXA gives a highly accurate reading of body fat percentage when compared to hydrostatic weighing.[26,55,57 The scan takes 20 minutes and is one that can be administered to children, the elderly or those with physical limitations. Another advantage is that unlike hydrostatic testing, DEXA takes into consideration differences in bone mass which can vary based on ethnicity and activity levels and is less affected by varying levels of hydration in the subject tested. [58] That said, it is not perfect as variation in fat distribution and front to back thickness of the person being scanned can affect the accuracy of DEXA estimates of soft tissue.[32]
There are other forms of body fat testing such as Near-Infrared Interactance, which is a method developed by the USDA to measure body composition in livestock based on infra-red light absorption and reflection, but its accuracy is not high enough that it is seriously considered for testing purposes. At the end of the day, very few people really need a body fat percentage test and such tests can only give an estimate at best whereas you can easily look in the mirror to monitor your progress and see how you feel to know if you are where you need to be. So don’t get too hung up on the numbers and remember that building muscle is key if you are trying to get that look!

{kind=link}
{kind=link}

High Intensity Bodyweight Training: Ballistic Pushups & Dips!
This was a tough one!
Starts out with ballistic push ups (like clap pushups but without the clap as my wrist is still not 100%) nonstop for 20 reps, then all out on dips for 10 reps.
To say it was painful would be an understatement, but you just have to push through and keep on going.
Still training, hope you are too and as always, Excelsior!!! #naturallyintense
#hometraining #homeworkout #homeworkout #highintensitytraining #naturalbodybuilder #naturalbodybuilding #fitover40 #naturalbodybuildingvideos #chestday #chesttraining #naturalbodybuildingtips #pushups #dips #bodyweighttraining #highintensitytrainingtips #drugfreebodybuilding #calesthenics
{kind=link}
Kevin's Unconventional Biceps Training- 3-6 Minutes a Week!
In this video I go over my biceps training using the Naturally Intense High Intensity Training protocols that helped me go from having arms measuring 11.5 to 12 inches to 18 inches drug free!
It's an unconventional approach for certain, but it's one that's helped my arms grow and the hundreds of men and women I have trained over the past 30 plus years.
Now, my success isn't due to being genetically gifted, as it took me the better part of 11 years to get my arms up to those measurements.
Which is significant as it works and been been proven time and time again to work for the average man or woman trying to grow their arms without drugs.
It's my hope that these high intensity training protocols can help you as much as they helped me!
Click on my bio link to see the full video on my YouTube channel and thanks as always for taking the time to look at my work!!! Excelsior!!! #naturallyintense
#highintensitytraining #naturalbodybuilder #naturalbodybuilding #fitover40 #naturalbodybuildingvideos #armworkout #bicepsworkout #naturalbodybuildingtips #biceps #armtraining #highintensitytrainingtips #drugfreebodybuilding #barbellcurls
{kind=link}
At the Lancaster Classic Day 2 Elimination Rounds Against European Champion, and World Record Holder Leo Pettersen @leo_barebow_archer
I don't talk much about it but I'm also a competitive barebow archer (surprise!) and last Saturday I had the honor of making it to Day 2 at the Lancaster Archery Classic in the Barebow Division, as I made the top 64 out of 267 competitors and had a chance to shoot with some of the greatest barebow shooters on the planet!
I didn't make it past Leo, but it was a real rush to be there and a huge thanks to my coach, Joe MyGlyn @prolinearchery for helping me get there.
Thanks as well to my good friend @sean_chan33 for all of his help from the very start, to my line buddy Aaron Shea for taking the shot and showing up to support!
My thanks as well to rob_kaufhold for putting on and promoting one of the best archery tournaments on earth!
Thanks also to to everyone who took the time to send a supporting word and I am looking forward to next year!!! #naturallyintense #barebow
#lancasterclassic #lancasterarcheryclassic2024 #lancasterarchery #archery #fitover40 #barebowrecurve #targetarchery
{kind=link}
Dumbo, Brooklyn circa 2004
This shot was taken as part of the promotion for my Naturally Intense DVD and was about a year after my last bodybuilding competition.
It was a grueling photoshoot.
We started at about 10 am and finished around 4pm and I was completely spent, but the more we shot the sharper I looked, so we kept on going.
It's nice to look back from time to time and as tired as I was, we all had a blast!
My thanks to @stephanie_corne_artwork, @https://pulse.ly/itgnag2dec and @ftaz1 for taking the shots!!!
Thanks for watching and as always, Excelsior!!! #naturallyintense
#naturalbodybuilder #naturalbodybuilding #throwback #fifthavenuegym #5thavenuegym #drugfreebodybuilding #naturalbodybuildinglifestyle #gymlife #gymmotivation #naturalbodybuildingmotivation #bodybuilding #blackandwhite #instablackandwhite #bnw
{kind=link}
Can You Build An Impressive Physique Training Only At Home?
Absolutely!
I stopped training in commercial gyms as of March 2020 and have been training at home ever since.
Initially I was admittedly worried that I might lose some of my gains or not make as much progress, but that certainly wasn't the case.
I've consistently continued to improve with my high intensity workouts and muscles have no idea where they are training.
As long as the criteria of adequate intensity and overload are met, there will be an adaptive response and your muscles will get bigger and stronger.
So don't worry at all about where you train, focus instead of what will be the best way for you to always be training!
Thanks for watching and as always, Excelsior!!! #naturallyintense
{kind=link}
Kevin's Three Day Training Spilt!
For the past 33 years I have trained three times a week with Naturally Intense High Intensity Training workouts lasting 10, 15 to 20 minutes max.
It's a training split tried and testes not only in it's helping me realize my goal of becoming a successful natural bodybuilder, but it's also helped hundreds of men and women over the past three decades.
I have tested just about every possible training split imaginable and for this particular style of high intensity training, this particular grouping consistently yields fantastic results.
I hope it helps you as much as it's helped me over the years and thanks so much for taking the time to look at my work.
Keep training hard and Excelsior!!! #naturallyintense
Excelsior!!! #naturallyintense
#trainingsplit #3daytrainingsplit #threedaytrainingsplit #naturalbodybuilding #naturalbodybuilder #naturalbodybuildingvideo #naturalbodybuildingmotivation #naturalbodybuildingtips #drugfreebodybuilding #bodybuilding #highintensitytraining #highintensitytrainingtips
{kind=link}
405 Stiff Leg Deadlift for 7 Reps! High Intensity Training.
First leg workout of the year and already pushing it!
I haven't done a stiff leg deadlift over 315lbs for about 3 years at this point, and I did my last set with 315lbs and comfortably got to 10 reps and decided I had far too much gas left in the tank and that I should go up in weight.
So I did.
I figured I might get a solid 6 reps in, but I made it to 7 and I think I could have gone on to get a full 10 reps BUT that's when good judgement prevailed.
As a bodybuilder having not trained this heavy for so many years, the shock of this much weight would be more than enough to stimulate muscle growth, and doing more reps wouldn't yield any greater returns, only increase the likelihood of injury.
It's not about the numbers, it's about training to a point where you achieve your goal, and it's important to have a goal in mind as a bodybuilder based on increasing muscle mass rather than hitting a particular number.
Besides, if in my 20's I never did more than 405lbs on a stiff leg deadlift, it doesn't make any sense going heavier than when I am almost 50!
Could I deadlift more at this point?
Absolutely but just because you can doesn't mean you should!
So keep those weights in a good working range, keep it safe and as always Excelsior!!! #naturallyintense
#hometraining #homeworkout #homeworkout #roguerack #highintensitytraining #naturalbodybuilder #naturalbodybuilding #fitover40 #naturalbodybuildingvideos #backworkout #naturalbodybuildingtips #backtraining #highintensitytrainingtips #drugfreebodybuilding #fitoverforty #deadlift
{kind=link}
Turning 50 in a few months...
Not much of a big deal for me as I still feel pretty much the same but I hope that my example helps show what can be done with a lifetime commitment to eating well and training consistently!
Thanks for coming along on the journey and as always, Excelsior!!! #naturallyintense
#naturalbodybuilder #naturalbodybuilding #healthylifestyle #fitover40 #drugfreebodybuilding #naturalbodybuildingmotivation #natty #fitness
Please note that all material is copyrighted and DMCA Protected and can be reprinted only with the expressed authorization of the author.

Featured everywhere from the Wall Street Journal to CBS News, Kevin Richardson’s Naturally Intense High Intensity Training have helped hundreds lose weight and transform their bodies with his 10 Minute Workouts. One of the top natural bodybuilders of his time, Kevin is also the international fitness consultant for UNICEF and one of the top personal trainers in New York City.
If You Liked This Post Then Check Out These Related Articles:
How Long Does It Take To Get Muscle Definition
The Evolutionary Argument Against Being Skinny
Why Do Men & Women Lose Body Fat Differently
5 Ways To Deal With Loose Skin After Weight Loss
How To Use A Scale Without Negatively Affecting Body Image
How Calories Relate To Weight Loss
References:
1. Wang J, Pierson RN, Heymsfield SB. The five level model: a new approach to organizing body composition research. Am J Clin Nutr 1992
2. Brozek J, Grande F, Anderson JT, Keys A. Densitometric analysis of body composition: revision of some quantitative assumptions. Ann NY Acad Sci 1963
3. Siri WE. Body composition from fluid spaces and density: analysis of methods. In: Brozek J, Henschel A, editors. Techniques for measuring body composition. Washington, DC: National Academy of Sciences, 1961
4. Baumgartner RN, Heymsfield SB, Lichtman S, Wang J, Pierson RN. Body composition in elderly people: effect of criterion estimates on predictive equations. Am J Clin Nutr 1991
5. Lohman TG. Advances in body composition assessment. Current issues in exercise science series (monograph 3). Champaign, IL: Human Kinetics, 1992.
6. Williams DF, Going SB, Massett MP, Lohman TG, Bare LA, Hewitt MJ. Aqueous and mineral fractions of the fat-free body and their relation to body fat estimates in men and women aged 49-82 years. In Ellis KJ, Eastman JD, editors. Human body composition: in vivo methods, models, and assessment. New York, NY: Plenum, 1992
7. Steinberger, J. et al. Comparison of body fatness measurements by BMI and skinfolds vs dual energy X-ray absorptiometry and their relation to cardiovascular risk factors in adolescents. Int. J. Obes.2005.
8. Sun, Q. et al. Comparison of dual-energy x-ray absorptiometric and anthropometric measures of adiposity in relation to adiposity-related biologic factors. Am. J. Epidemiol.2010.
9. Lawlor, D.A. et al. Association between general and central adiposity in childhood, and change in these, with cardiovascular risk factors in adolescence: prospective cohort study. BMJ 2010.
10. Flegal, K.M. & Graubard, B.I. Estimates of excess deaths associated with body mass index and other anthropometric variables. Am. J. Clin. Nutr.2009
11. Freedman, D.S. et al. Relation of body mass index and skinfold thicknesses to cardiovascular disease risk factors in children: the Bogalusa Heart Study. Am. J. Clin. Nutr.2009
12. Willett, K. et al. Comparison of bioelectrical impedance and BMI in predicting obesity-related medical conditions. Obes. (Silver Spring) 2006
13. Centers for Disease Control and Prevention. Body Mass Index: Considerations for Practitioners.
14. Prentice, A.M. & Jebb, S.A. Beyond body mass index. Obes. Rev. 2001
15. Centers for Disease Control and Prevention. Body Mass Index: About BMI for Adults 2015
16. Wagner, D.R. & Heyward, V.H.. Measures of body composition in blacks and whites: a comparative review. Am. J. Clin. Nutr 2000.
17. Flegal, K.M. et al. High adiposity and high body mass index-for-age in US children and adolescents overall and by race-ethnic group. Am. J. Clin. Nutr. 2010
18. Barba, C. et al. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004.
19. Orphanidou C, McCargar L, Birmingham CL, Mathieson J, Goldner E. Accuracy of subcutaneous fat measurement: comparison of skinfold calipers, ultrasound, and computed tomography. J Am Diet Assoc. 1994
20. Kostek MA1, Pescatello LS, Seip RL, Angelopoulos TJ, Clarkson PM, Gordon PM, Moyna NM, Visich PS, Zoeller RF, Thompson PD, Hoffman EP, Price TB. Subcutaneous fat alterations resulting from an upper-body resistance training program. Med Sci Sports Exerc. 2007
15. KROTKIEWSKI, M., A. ANIANSSON, G. GRIMBY, P. BJORNTORP, and L. SJOSTROM. The effect of unilateral isokinetic strength training on local adipose and muscle tissue morphology, thickness, and enzymes. Eur. J. Appl. 1979.
21. TREUTH, M. S., G. R. HUNTER, T. KEKES-SZABO, R. L. WEINSIER, M. I. GORAN, and L. BERLAND. Reduction in intra-abdominal adipose tissue after strength training in older women. J. Appl. Physiol. 1995.
22. TREUTH, M. S., A. S. RYAN, R. E. PRATLEY, et al. Effects of strength training on total and regional body composition in older men. J. Appl. Physiol. 1994
23. Mazess RB, Barden HS, Bisek JP, Hanso, J. Dual-energy x-ray absorptiometry for total-body and regional bone-mineral and soft-tissue composition. Am J Clin Nutr 1990
24. Callaway CW, Chumlea WC, Bouchard C, Himes JH, Lohman TG, Martin AD, et al. Circumferences. In Lohman TG, Roche AF, Martorell R, editors. Anthropometric standardization reference manual. Champaign, IL: Human Kinetics, 1988
25. Going SB, Massett MP, Hall MC, Bare LA, Root PA, Williams DP, et al. Detection of small changes in body composition by dual-energy x-ray absorptiometry. Am J Clin Nutr 1993
26. Friedl KE, DeLuca JP, Marchitelli LJ, Vogel JA. Reliability of body-fat estimations from a four compartment model by using density, body water, and bone mineral measurements. Am J Clin Nutr 1992
27. Prior BM, Cureton KJ, Modlesky CM, Evans EM, Sloniger MA, Saunders M, et al. In vivo validation of whole body composition estimates from dual-energy x-ray absorptiometry. J Appl Physiol 1997
28. Kohrt WM. Body composition by DXA: tried and true? Med Sci Sports Exerc 1995
29. Hart PD, Wilkie ME, Edwards A, Cunningham J. Dual energy x-ray absorptiometry versus skinfold measurements in the assessment of total body fat in renal transplant recipients. Eur J Clin Nutr 1993
30. Wang J, Thornton JC, Russell M, Burastero S, Heymsfield S, Pierson RN. Asians have lower body mass index (BMI) but higher percent body fat than do whites: comparison of anthropometric measurements. Am J Clin Nutr 1994
31. Wang J, Thornton JC, Burastero S, Heymsfield S, Pierson RN. Bioimpedance analysis for estimation of total body potassium, total body water, and fat-free mass in white, black, and Asian adults. Am J Hum Biol 1995
33. Harrison GG, Buskirk ER, Lindsay Carter JE, Johnston FE, Lohman TG, Pollock ML, et al. Skinfold thicknesses and measurement technique. In Lohman TG, Roche AF, Martorell R, editors. Anthropometric standardization reference manual. Champaign, IL: Human Kinetics, 1988
34. Lohman TG, Pollock ML, Slaughter MH, Brandon LJ, Boileau RA. Methodological factors and the prediction of body fat in female athletes. Med Sci Sports Exerc 1984
35. Friedl, KE; Moore RJ; Martinez-Lopez LE; Vogel JA; Askew EW; Marchitelli LJ; Hoyt RW; Gordon CC (August 1994). “Lower limit of body fat in healthy active men”. J Appl Physiol.
36. Heymsfield S, Lohman T, Wang Z, Going S. Human Body Composition. 2nd ed. Champaign, IL: Human Kinetics; 2005
37. University of Pennsylvania Body Composition Information and FAQ’s Sheet
38. MacLean PS, Bergouignan A, Cornier MA, Jackman MR. Biology’s response to dieting: the impetus for weight regain. Am J Physiol Regul Integr Comp Physiol. 2011
39. Hall KD. Computational model of in vivo human energy metabolism during semistarvation and refeeding. Am J Physiol Endocrinol Metab. 2006
40. Kim JY, Han SH, Yang BM. Implication of high-body-fat percentage on cardiometabolic risk in middle-aged, healthy, normal-weight adults. Obesity (Silver Spring). 2013
41. Bray GA. Classification and evaluation of the obesities. Med Clin North Am 1989
42. Inoue S, Zimmet P, Caterson I, Chunming C, Ikeda Y, Khalid A. WHO/IASO/IOTF. The Asia-Pacific perspective: redefining obesity and its treatment. Sydney (Australia): Australasian Society for the Study of Obesity; 2000.
43. Lee DY, Choi ES, Kim JH, et al. Comparison of the predictability of cardiovascular disease risk according to different metabolic syndrome criteria of American Heart Association/National Heart, Lung, and Blood Institute and International Diabetes Federation in Korean Men. Korean Diab J 2008
44. Deurenberg-Yap M, Chew S, Deurenberg P. Elevated body fat percentage and cardiovascular risks at low body mass index levels among Singaporean Chinese, Malays and Indians. Obes Rev 2002.
45. Kishimoto N, Okita K, Takada S, et al. Lipoprotein metabolism, insulin resistance, and adipocytokine levels in Japanese female adolescents with a normal body mass index and high body fat mass. Circ J 2009
46. Ito H, Nakasuga K, Ohshima A, et al. Excess accumulation of body fat is related to dyslipidemia in normal-weight subjects. Int J Obes Relat Metab Disord 2004
47. Tanaka S, Togashi K, Rankinen T, et al. Is adiposity at normal body weight relevant for cardiovascular disease risk? Int J Obes Relat Metab Disord 2002
48. Han JH, Kim SM. Relationship between percent body fat and cardiovascular risk factors for normal weight adults. J Korean Acad Fam Med 2006
49. Heyward V. ASEP methods recommendations: Body composition assessement. Journal of Exercise Physiology 2001
51. Jackson AS, Pollock ML. Generalized equations for predicting body density in men. Br J Nutr 1978
52.Katch FI, Katch VL. Measurement and prediction errors in body composition assessment and the search for the perfect equation. Res Q Exerc Sport 1980
53. Behnke AR, Wilmore JH. Evaluation and regulation of body build and composition. Englewood Cliffs, NJ: Prentice Hall, 1974.
54. Bonge D, Donnelly JE. Trials to criteria for hydrostatic weighing at residual volume. Res Q Exerc Sport 1989
55.Going SB, Massett MP, Hall MC, Bare LA, Root PA, Williams DP, et al. Detection of small changes in body composition by dual-energy x-ray absorptiometry. Am J Clin Nutr 1993
57. Prior BM, Cureton KJ, Modlesky CM, Evans EM, Sloniger MA, Saunders M, et al. In vivo validation ofwhole body composition estimates from dual-energy x-ray absorptiometry. J Appl Physiol 1997
58. Kohrt WM. Body composition by DXA: tried and true? Med Sci Sports Exerc 1995
60. McCrory MA, Gomez TD, Bernauer EM, Mole PA. Evaluation of a new air displacement plethysmograph for measuring human body composition. Med Sci Sports Exerc 1995
61. Wagner, DR, Heyward VH, Gibson AL. Validation of air displacement plethysmography for assessing body composition. Med Sci Sports Exerc 2000
62. Collins MA, Millard-Stafford ML, Sparling PB, Snow TK, Rosskopf LB, Webb SA, et al. Evaluation of the Bod Pod for assessing body fat in collegiate. Med Sci Sports Exerc. 1999